Reviews
Friedrich Anderhuber, Ulrike Pilsl
Soft tissues of the face – Part 2: the connective tissue
Keywords | Summary | Correspondence | References
Keywords
Connective tissue, fascia, septa, SMAS
Schlüsselworte
Summary
In contrast to epithelial tissue, which is found on almost all external and internal body surfaces, connective tissue consists of significantly fewer cells and much more intercellular substance, also called extracellular matrix. The connective tissue in the facial area is present in the form of fascia (fascia parotideomasseterica, fascia temporalis), as SMAS (superficial musculo-aponeurotic system), in the form of retaining ligaments (retinacula cutis) and as septa.
Zusammenfassung
The connective tissue in the facial area is present in the form of fascia (fascia parotideomasseterica, fascia temporalis), as SMAS (superficial musculo-aponeurotic system), in the form of retaining ligaments (retinacula cutis) and as septa.
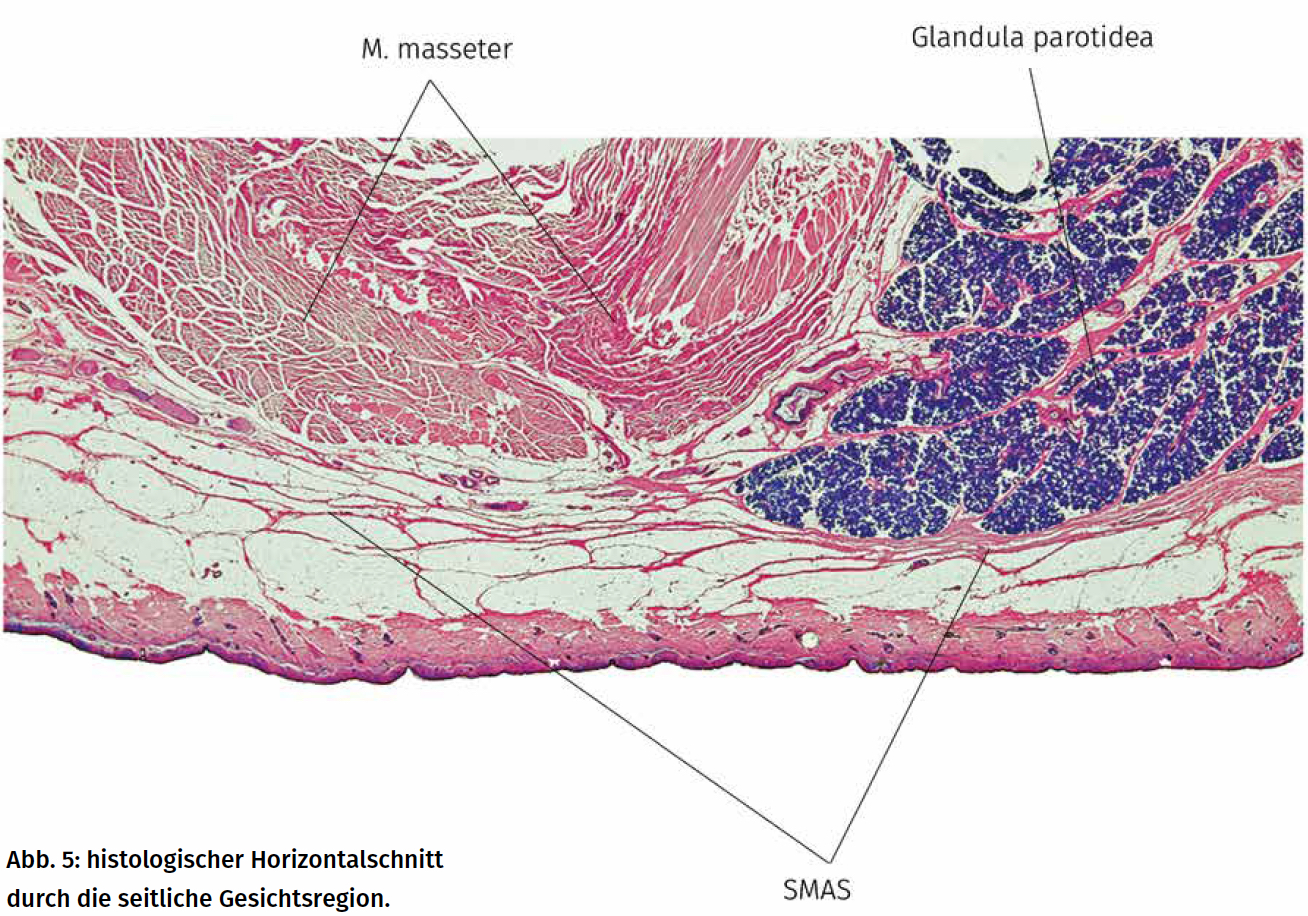
The SMAS (Fig. 1) is a structure with connective tissue and muscular (platysma, mimic musculature) components. If the integument of the face is divided into 3 layers (cutis, subcutis and fascia), the SMAS belongs to the third layer [1]. This third layer can be mobilized as a whole from the neck to the temple. The SMAS is present in the area of the parotid gland as a tight connective tissue plate that is fused with the parotid fascia but can be separated from it. A sliding layer can thus be created between the SMAS and the underlying fascia of the parotid gland and the masseter muscle in the midface area, in which the SMAS can be pulled against the support. The further forward you follow the SMAS, the more its plate-like structure is lost, so that the SMAS is fragmented in the front of the face and envelops the mimic musculature. Together with muscle fibers of the mimic musculature, the splintered SMAS radiates into the dermis. Above the zygomatic arch, the SMAS continues into the galea aponeurotica, the flat tendon of the epicranius muscle. In the temporal region, the galea aponeurotica is usually referred to as the fascia temporoparietalis or the fascia temporalis superficialis, which often leads to confusion regarding the fasciae.
This often leads to confusion regarding the fascial relationships of the temporal region.
A distinction is made between “true” (osteocutaneous) retaining ligaments of the face (retinacula cutis) (Fig. 2), which originate from the periosteum, often in the area of sutures, and “false” (fasciocutaneous) retaining ligaments, which originate from the fascia or the SMAS [2]. Both forms radiate into the dermis. The retaining ligaments of the face are not ligaments in the anatomical sense as in the joints, but rather less structured fiber compactions. The osteocutaneous retaining ligaments include the zygomatic ligaments, the orbital retaining ligaments, the maxillary part of the buccomaxillary ligaments, the mandibular retaining ligaments, the platysma-mandibular ligaments and the submental ligaments.

The zygomatic ligaments (McGregor’s patch) have their densest origin in the area of the sutura temporozygomatica, but also originate further back from the zygomatic arch. The orbital suspensory ligaments originate at the supra- and infraorbital margo and must penetrate the orbicularis oculi muscle in order to reach the dermis. They are most strongly developed in the area of the sutura frontozygomatica. The lower part of the orbital retaining ligaments, which originates from the margo infraorbitalis, is also known as the orbito-malar septum. The maxillary part of the bucco-maxillary ligaments originates in the area of the zygomaticomaxillary sutura and radiates into the dermis of the nasolabial fold. The mandibular retaining ligaments originate in the anterior third of the mandible, approximately 1 cm above its lower edge, in front of the origin of the depressor anguli oris muscle. The platysma-mandibular ligaments originate from the lower edge of the corpus mandibulae lateral to the mandibular ligaments and must pass through the platysma in order to reach the dermis. In the chin area, the submental ligaments arise from the lower edge of the mandibular body. However, these can often be absent. The fasciocutaneous retaining ligaments have a loose, lattice-like structure. They include the platysma-auricular ligaments, the septum subcutaneum parotideomassetericum, the buccal part of the bucco-maxillary ligaments and the masseter-cutaneous retaining ligaments.
The platysma-auricular ligaments originate from the SMAS and the fascia parotideomasseterica in the area of the posterior edge of the platysma in front of the ear. They must also pass through the platysma in order to reach the dermis. The septum subcutaneum parotideomassetericum [3] also originates at the SMAS in the area of the parotid gland and runs anteriorly and laterally into the buccal skin. The masseter-cutaneous ligaments originate from the SMAS at the anterior edge of the masseter muscle. The buccal part of the buccomaxillary suspensory ligaments originates from the buccal mucosa, breaks through the buccinator muscle and radiates into the dermis of the nasolabial fold.
Address of Correspondence
Dr. med. Ulrike Pilsl
Institut für Anatomie, MUG
Harrachgasse 21
AT-8010 Graz
ulrike.pilsl@meduni-graz.at
Conflict of Interests
None.
References
1. Cotofana S, Redka-Swoboda W (2014) Die Anatomie des Superfiziellen Musculo-Aponeurotischen Systems (SMAS). Kosm Med 35(5): 224–233.
2. LaTrenta G (2004) Atlas of Aesthetic Face & Neck Surgery. Saunders.
3. Pilsl U, Anderhuber F (2010) The Septum Subcutaneum Parotideomassetericum.
Dermatol Surg 36: 2005–2008.