Reviews
Friedrich Anderhuber, Ulrike Pilsl
Soft tissues of the face – part 1: The musculature
Keywords | Summary | Correspondence | References
Keywords
masticatory musculature, mimic musculature, soft tissues of the face
Schlüsselworte
Summary
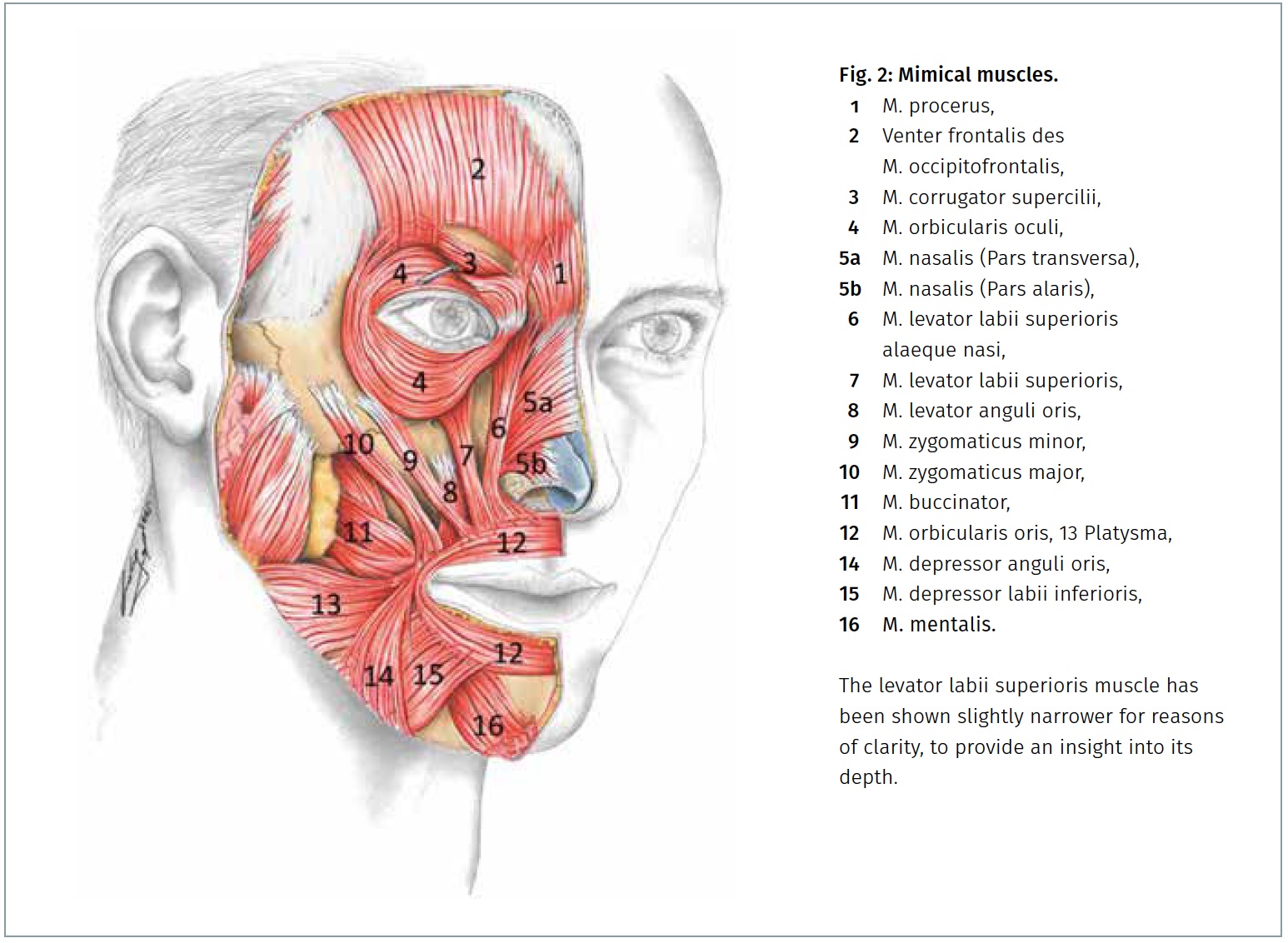
The mimic muscles are innervated by branches of the facial nerve. Most of the muscles originate in the bones of the skull or in the overlying subcutis, to which they are connected by elastic end tendons. The mimic muscles lie without fascia in the subcutaneous fat tissue, with the exception of the buccinator muscle, which is covered by the fascia buccopharyngea. The facial muscles are described in detail here.
Zusammenfassung
The head and face are anatomically divided into several regions (Fig. 3). On the head, a distinction is made between several capitis regions: the frontal region, the temporal region, the parietal region and the occipital region, the parietal region and the occipital region. When categorising the facial regions, a subdivision can be made into a regio faciei medialis and lateralis. The regio faciei medialis includes the regio orbitalis, the regio nasalis, the regio infraorbitalis, the regio oralis and the regio mentalis. The regio faciei lateralis includes the regio zygomatica, the regio buccalis and the regio parotideomasseterica [5]. In common parlance, the face extends to the hairline, so the forehead is included in the face. As is the case almost everywhere on the skull, the bones of the face are covered by relatively few soft tissues, so that the bony base of the face is palpable in many places and the vessels and nerves run relatively superficially.
The soft tissues of the face have an onion-skin-like structure. Immediately beneath the skin lies the superficial fatty tissue and below this the superficial musculo-aponeurotic system (SMAS), which envelops the mimic musculature. Between and below the facial muscles is the deep fat and below this the layer of blood vessels, nerves and the parotid duct. Another layer deeper is the corpus adiposum buccae (Bichat) and beneath it the bones of the facial skull.
Two muscle groups can be found in the facial area: the masticatory muscles (Mm. masticatorii) and the mimic muscles (Mm. faciei).
The masticatory muscles originate from the 1st pharyngeal arch (mandibular arch), whose associated nerve is the trigeminal nerve. These muscles are therefore innervated by the motor part of the 3rd trigeminal nerve, the masticatory nerve of the mandibular nerve. The masseter muscle, the temporalis muscle, the medial pterygoid muscle and the lateral pterygoid muscle belong to the masticatory muscles. The two pterygoid muscles are located in the deep lateral facial region in the infratemporal fossa and are closely related to the corpus adiposum buccae (Bichat). The temporalis muscle originates from the planum temporale and the temporal fascia covering it and attaches to the coronoid process and mandibular ramus with a strong tendon. The masseter muscle originates with a superficial part from the lower edge and a deep part from the inner surface of the zygomatic arch and attaches to the outer surface of the mandibular branch and the mandibular angle. It is largely covered by the parotid gland (glandula parotidea) and is involved in jaw closure together with the temporalis muscle and the medial pterygoid muscle.

The mimic musculature originates from the 2nd pharyngeal arch (hyoid arch). In the course of embryonic development, it leaves its original position in the area of the hyoid arch and spreads over the entire face. It is innervated by the nerve of the 2nd pharyngeal arch, the facial nerve. Its branches run between the superficial and deep muscles so that the nerves reach the superficial muscles from the underside. The mimic musculature has several differences to the striated skeletal musculature of the rest of the body: one major difference is that the mimic musculature is not localised under the subcutis, but is embedded between the superficial and deep subcutaneous fat layer and therefore has a subcutaneous location, which in turn means that these are “skin muscles”. A further difference to the skeletal musculature is that although the mimic musculature also originates from the bone, it does not attach to the bone but – together with the extensions of the SMAS – usually radiates into the dermis in a fan shape. This causes furrows and wrinkles to form when the individual muscles contract, resulting in different facial expressions.
A third difference lies in the fact that the mimic musculature is enveloped by an epimysium and surrounded by extensions of the SMAS, but does not have its own muscle fascia, as is usually the case on the body. Furthermore, the facial musculature differs from the skeletal musculature in that the mimic musculature does not form a uniform layer, but is present in 3 layers, between which there are gaps in which the deep fatty bodies of the face are embedded. The superficial layer contains the venter frontalis of the occipitofrontalis muscle, the procerus muscle, the orbicularis oculi muscle, the nasalis muscle, the zygomaticus minor muscle, the orbicularis oris muscle, the risorius muscle, the depressor anguli oris muscle and the platysma.
The venter frontalis of the occipitofrontal muscle originates in the skin of the eyebrows and the glabella and connects here with fibres of the orbicularis oculi muscle. It runs slightly diverging upwards and then merges into its tendon, the galea aponeurotica. Its contraction causes transverse wrinkles on the forehead on the one hand and raises the eyebrow and upper eyelid on the other.
The procerus muscle originates from the nasal bone and attaches to the skin of the glabella. Its contraction creates transverse folds at the root of the nose and at the same time it acts antagonistically to the medial part of the venter frontalis of the occipitofrontalis muscle by lifting the transverse folds on the forehead.
The orbicularis oculi muscle consists of 3 parts: the pars palpebralis originates from the superficial rein of the medial palpebral ligament and the anterior lacrimal crest and attaches to the lateral palpebral ligament. It is responsible for the smooth blinking and closure of the eyelid, which are important for the distribution of tear fluid. The pars orbitalis joins the pars palpebralis peripherally and has its origin next to the lig. palpebrale mediale on the frontal process of the maxilla and on the pars nasalis of the frontal bone. Its insertion lies in the skin of the eyebrow, the temple and the cheek. The pars orbitalis therefore has neither a bony attachment nor an attachment to the lateral palpebral ligament. It is important for squinting the eyes, resulting in radial skin folds (“crow’s feet”) at the lateral corner of the eye. The pars lacrimalis originates at the deep rein of the medial palpebral ligament, at the posterior lacrimal crest and at the lacrimal fascia, but then runs directly along the lid margin and attaches to the lateral palpebral ligament. It is important for tear drainage by promoting the pumping mechanism and also counteracts lengthening of the bulb due to its tone.
The nasalis muscle originates at the juga alveolaria of the lateral incisor and the canine of the maxilla and attaches to the nasal wings with a pars alaris; with a pars transversa it reaches the cartilago nasi lateralis and connects to the tendon plate of the muscle on the opposite side. The pars alaris (= dilator naris muscle) widens the nostril, the pars transversa (= compressor naris muscle) narrows it.
The zygomaticus minor muscle originates from the zygomatic bone and also draws its fibres from the pars orbitalis of the orbicularis oculi muscle. It radiates into the skin of the nasolabial groove and intertwines with the fibres of the orbicularis oris muscle in the area of the upper lip. It pulls the corner of the mouth and the nasolabial furrow laterally and upwards.
The orbicularis oris muscle forms the muscular basis of the lips and is firmly fused to the skin. It is not actually a ring muscle as its name incorrectly describes, but consists of 4 parts. Its origin lies in the area of the juga alveolaria of the maxilla and mandible at the level of the incisors. The part around the oral cleft is called the pars marginalis and bends outwards in a hook shape in the area of the red of the lips. The adjoining peripheral part of the orbicularis oris muscle is the labial pars. This extends cranially to the nasal septum and caudally to the lip-chin furrow (sulcus mentolabialis). In the area of the corner of the mouth, its fibres intertwine with the muscles radiating in from above, laterally and below to form a nodular thickening, the modiolus anguli oris.
The orbicularis oris muscle is responsible for closing the oral fissure and the trunk-like protrusion of the lips and is therefore involved in many complex movements of the mouth that are necessary for food intake, speaking, etc. Muscle fibres branch off from the cranial edge of the muscle, which run to the skin of the nasal septum and are known as the depressor septi muscle. This muscle can pull the nasal septum downwards and thus widen the nostrils.
The risorius muscle is a relatively inconstant and usually weak muscle that originates from the parotid fascia and the skin of the cheek and radiates into the corner of the mouth. It can also be present as a separation of the platysma or the zygomaticus major muscle. It widens the oral cleft and is responsible for the “cheek dimple”.
The depressor anguli oris muscle has a broad origin on the lower edge of the mandible from the chin to the first molar. It attaches to the skin of the corner of the mouth and individual fibres radiate into the peripheral part of the pars labialis of the orbicularis oris muscle of the upper lip. Its contraction pulls the corner of the mouth and the upper lip downwards.
The platysma originates in the skin at the level of the 2nd rib and runs cranially as a thin plate. Its medial fibres attach to the lower jaw and intertwine with the fibres on the opposite side. A muscle-free triangle usually remains above the sternum. The lateral fibres of the platysma radiate into the cheek area, cover the lower part of the masseter muscle and the parotid gland and intertwine with other mimic muscles at the corner of the mouth. The platysma stretches the skin of the neck and forms longitudinal folds, it can lift the skin of the chest wall and is involved in pulling down the corners of the mouth.
The middle layer of the mimic musculature includes the zygomaticus major muscle, the levator labii superioris alaeque nasi muscle, the levator labii superioris muscle and the depressor labii inferioris muscle.
The zygomaticus major originates laterally from the zygomaticus minor from the zygomatic bone and radiates into the skin of the corner of the mouth. It thus participates in the elevation of the corner of the mouth.
The levator labii superioris alaeque nasi muscle originates from the frontal process of the maxilla and radiates into the skin of the nasal wing and the nasolabial furrow. It can lift the nostril and is involved in lifting the upper lip.
The levator labii superioris muscle originates directly below the infraorbital marrow and radiates into the skin of the upper lip. It also participates in the elevation of the upper lip. The latter three muscles form a continuous muscular plate.
The depressor labii inferioris muscle originates at the base of the mandible below and medial to the mental foramen, partially covered by the depressor anguli oris muscle, and runs medially upwards to radiate into the orbicularis oris muscle. Its contraction pulls the lower lip downwards.
The deep layer of the mimic musculature consists of the corrugator supercilii muscle, the levator anguli oris muscle, the buccinator muscle and the mentalis muscle. The corrugator supercilii muscle originates at the frontal bone above the root of the nose and radiates into the skin above the centre of the eyebrow. Its contraction creates vertical folds above the root of the nose.
The levator anguli oris muscle originates from the maxilla below the infraorbital foramen and radiates into the corner of the mouth. It participates in the elevation of the corner of the mouth.
The buccinator muscle forms the muscular basis for the cheek. It originates at the alveolar processes of the maxilla and mandible at the level of the 1st to 2nd molars and at the pterygomandibular raphe. Its fibres radiate into the corner of the mouth in such a way that the upper fibres run downwards and the lower fibres upwards and cross over each other in the area of the modiolus. Its contraction allows air to be pressed out of the mouth (blowing) and prevents the buccal mucosa from being trapped between the rows of teeth when chewing. It can also pull the oral fissure to the side.
The mentalis muscle originates from the juga alveolaria of the lower jaw at the level of the incisors and runs obliquely medially and downwards to the skin of the chin. When contracted, it pulls the chin skin upwards, creating the transverse mentolabial groove
and small dimples in the skin (“cobblestone chin”). Together with the orbicularis oris muscle, it can protrude the lower lip (“pucker”).
Address of Correspondence
Dr.med. Ulrike Pilsl
Institute of Anatomy, MUG
Harrachgasse 21
AT-8010 Graz
ulrike.pilsl@meduni-graz.at
Conflict of Interests
None.